Breast cancer: first scientifically validated guidelines on the usefulness of the imaging exam known as FDG PET/CT
Currently, the decision of whether or not to perform a nuclear medicine imaging exam called FDG PET/CT on breast cancer patients depends largely on each doctor's usual practice. The publication of scientifically validated guidelines, developed by an international and multidisciplinary team of experts, should make the use of this exam less empirical, for the benefit of patients.
Experts from two international nuclear medicine societies (EANM and SNMMI) have joined those from important societies of various other medical specialities involved in the care of breast cancer patients – including oncology, surgery, radio-oncology and breast imaging – to draw up a set of recommendations, based on scientific evidence, on the correct utilisation, in breast cancer, of a medical imaging exam. The exam in question has been used for several years and involves radioactive substances, in this case a glucose analogue called fluorodeoxyglucose (FDG).
Despite the fact that nuclear medicine specialists are primarily responsible for guaranteeing the quality of the results and of the interpretation of the exam, until now there were no official recommendations, with multidisciplinary validation by international societies, for the use of this hybrid technology. Now the situation has changed: the European Journal of Nuclear Medicine and Molecular Imaging has published the first guidelines with the participation of nuclear medicine experts.
Two of the 15 co-authors of the document are from the Champalimaud Foundation: Sofia Vaz, a specialist in nuclear medicine and a member of the oncology committee of the European Association of Nuclear Medicine; and Fátima Cardoso, an oncologist who heads the Foundation's Breast Unit and is the president of the Advanced Breast Cancer Global Alliance. The Breast Unit team already uses the imaging exam very frequently to support clinical decision-making at different stages of the disease.
This is a hybrid imaging exam because it contains two components: a PET scan, which allows the mapping of tumour sites where cells are proliferating, and a CT scan, which provides information on the structure of tumoural lesions. As for FDG, it is bound to a radioactive substance, fluorine-18 (18F). The amount of [18F]FDG administered intravenously is minimal, causes no effects on the body and no adverse effects are expected.
Since tumour cells that are dividing need energy to do so, this means that the tumour cells that pick up FDG are actively proliferating. PET/CT is a scan of the entire body, usually from the head to the knees. It is a safe, minimally invasive study (it only requires the injection of FDG), quick and easy to carry out, as the patient's position (usually lying on their back) and the duration of the scan (around 20 minutes on the equipment) can be relatively adapted according to each person's needs.
PET/CT is used in various non-oncological diseases; however, it is mainly used in the staging and follow-up of many cancers, and particularly in breast cancer. In European and North American countries, PET/CT is often used for "non special type" (NST) cancers, formerly known as invasive ductal carcinomas, which account for around 80 per cent of breast cancers. There are other types of breast cancer, for example, lobular and neuroendocrine subtypes, but in those cases, the benefit of the scan is not so well established.
FDG PET/CT scans prescribed at an early stage of breast cancer can have an impact on patient survival and quality of life. When performed at the right time, the exam makes it possible to avoid unnecessary treatments. Until now, multidisciplinary and internationally validated recommendations for the use of FDG PET/CT in breast cancer were lacking.
To formulate the recommendations, the authors of the document carried out an exhaustive review of the scientific literature on the different indications for FDG PET/CT in NST breast cancer. Then the experts voted to approve the recommendations and a consensus to clarify in which clinical situations FDG PET/CT should be performed was reached.
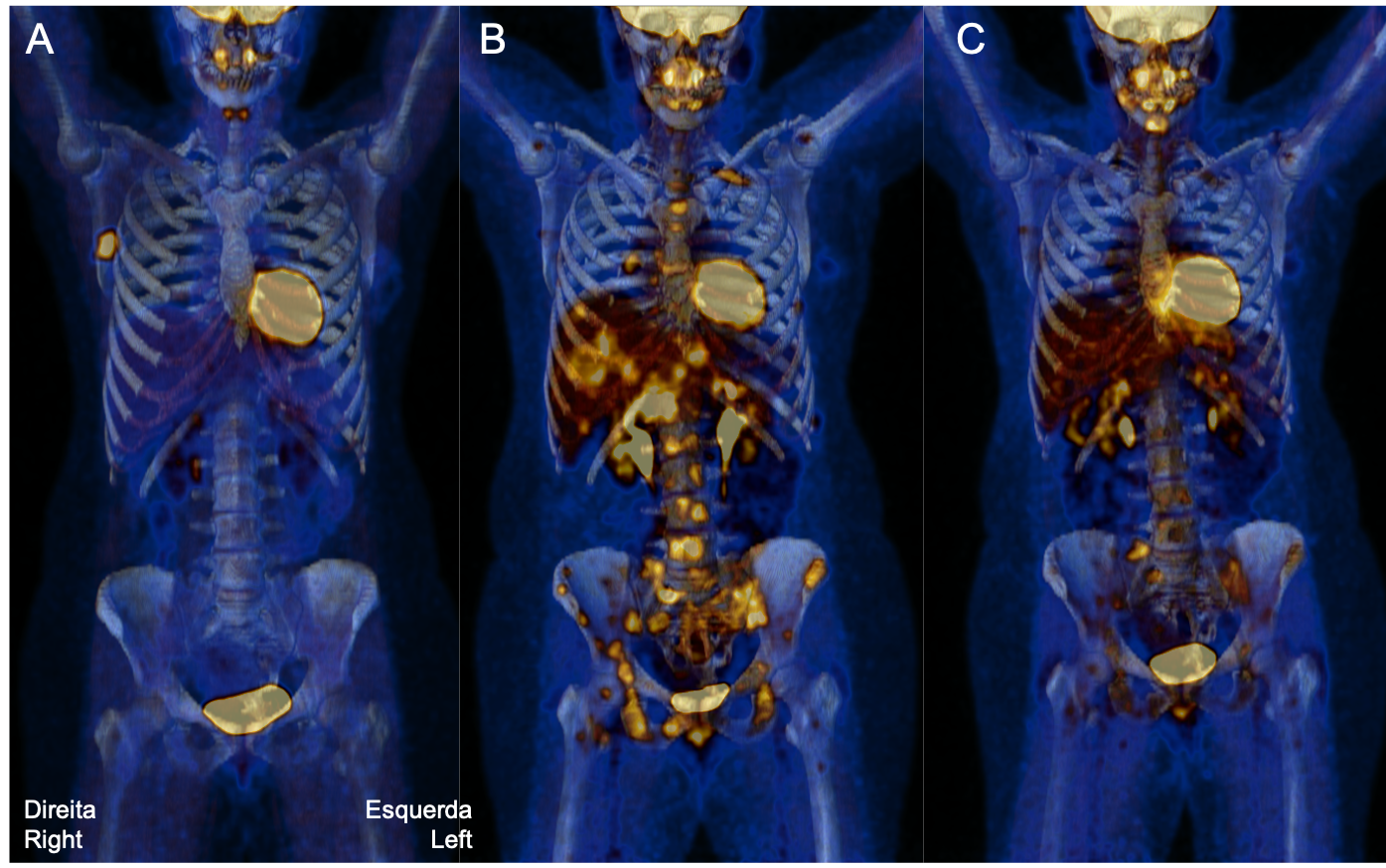
The group of experts approved recommendations in three main clinical situations. The first stipulates that patients with NST breast cancer at stage IIB (locally advanced cancer) or higher benefit from a FDG PET/CT scan for systemic staging of their cancer soon after diagnosis (see figure, image A). Locally advanced cancer is a cancer that has already progressed in the breast and possibly in nearby lymph nodes, but that, in principle, has not yet metastasised. The identification of distant tumour lesions (metastases) at this stage is key to deciding on the most effective treatment.
The second recommendation is that the FDG PET/CT scan is indicated for monitoring the response to treatment (see figure, image C). It makes it possible to assess, at an early stage, whether or not there is a response and thus helps determine the best treatment, thereby avoiding unnecessary toxicities. And third, the exam is also indicated for assessing the location and extent of lesions when the cancer relapses (see figure, image B).
The recommendations should be updated regularly or if new scientific evidence emerges. As technological advances make it possible to identify tumour cells at ever earlier stages, and sooner after treatment begins, studies will likely emerge concluding that PET/CT scanning may also be useful at stage IIA, and not just at IIB. In addition, several groups have investigated the semi-quantitative analysis of the intensity of FDG uptake by tumour lesions as a possible cancer biomarker.
With regard to the other types of breast cancer, new drugs are being discovered and evaluated [for use with PET/CT] that may become very important in the future. For example, fluoroestradiol (FES), which is an analogue of the hormone oestrogen, and fibroblast activation protein inhibitor (FAPI), which marks the fibroblasts that make up the tumour microenvironment, have shown very promising results in breast cancer, especially in the lobular subtype, but they need further clinical validation. In the future, the recommendations should also advance in this direction.
Image caption: An FDG PET/TCT scan from the same patient showing: in A, a tumour located in the right breast; in B, the location and extent of several lesions (in the liver and bones) when the cancer relapsed; and in C, the reduction of lesions in response to treatment (there is physiologic FDG uptake in the brain and heart, and urinary excretion with bladder accumulation). Image Credit: Nuclear Medicine - Radiopharmacology Department, Champalimaud Foundation.
Text by Ana Gerschenfeld, Health&Science Writer of the Champalimaud Foundation.